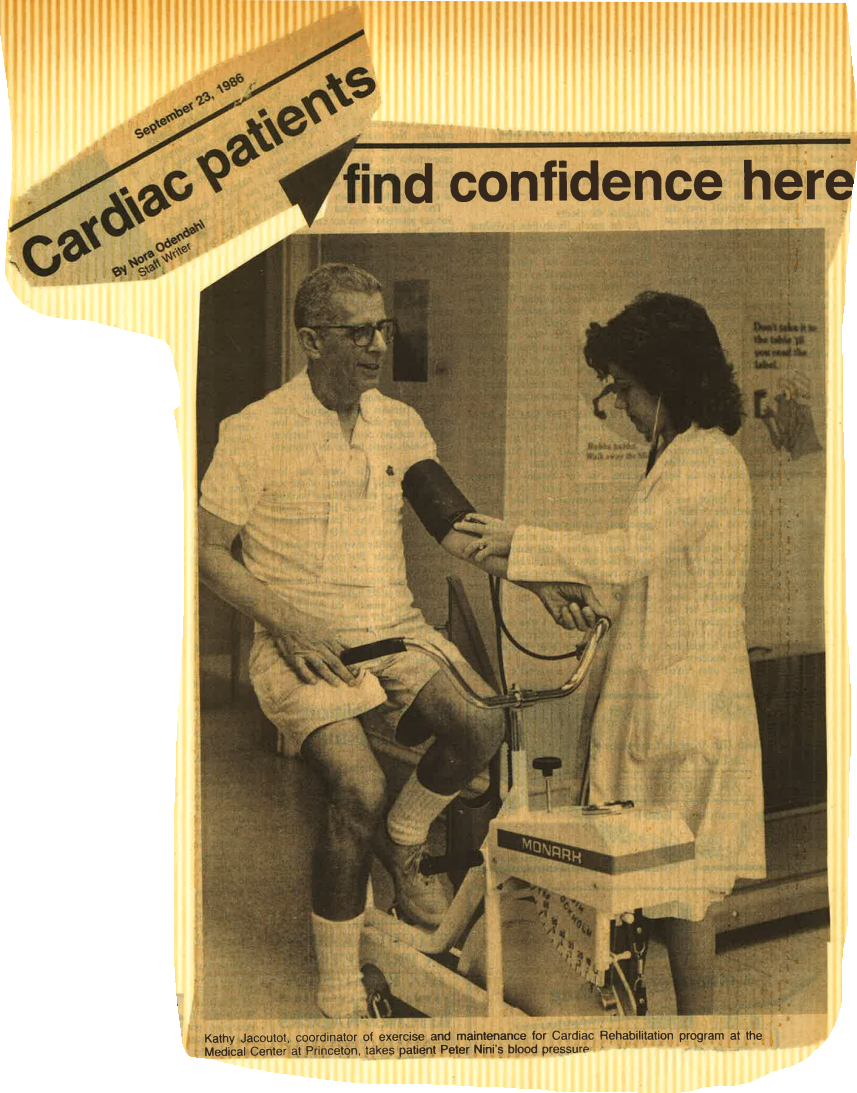
Kathy Jacoutot, coordinator of exercise and maintenance for Cardiac Rehabilitation program at the Medical Center at the Medical Center at Princeton, takes patient Peter Nini’s blood pressure.
23 September, 1986
Cardiac patients find confidence here
By Nora Odendahl
Staff Writer
Ms. Jacoutot mentioned that the Medical Center is working with the American Heart Association to develop – a Princeton-area chapter of the “Zipper Club.” a group of recovered heart ‘patients who offer emotional support to current cardiac patients. The volunteers, who take a training session. are matched to patients in age, sex, and diagnosis.
ONE GRADUATE of the rehabilitation program. Princeton resident Peter Nini. advises other patients. “There is life beyond a heart attack and open heart surgery.•• The journeyman glazier and volunteer firefighter suffered a massive heart attack and had unusual complications: four other near-attacks, bypass surgery, removal of a ventricular ancurisin and insertion of a pacemaker. In lune. four months after the heart attack. He entered the exercise and maintenance program. At the outset, walking left him short of breath; at the end of 12 weeks, 30-minute exercise periods had become routine.
Asked if he had felt apprehensive about starting an exercise program after his heart attack and surgery. Mr. Nini responded. “Quite to the contrary, I was looking forward to it. I needed something to give me some strength and weight back, and the therapy worked marvelously. I was very surprised at what could be achieved with a few minutes of one exercise and then a few minutes of another over a period of time.”
Mr. Nini is now lifting weights, walking and using an exercise bike, but, he said, “If I can get the insurance company to go along with me, I’ll come back for another 12 weeks of therapy.” (Most people come only for one 12—week program and then continue at home, returning perhaps for a monthly monitoring session.)
MR. NINI SAID that he, for one, had made changes in the habits that put him at risk for heart disease. “You really have no choice in the matter. Those changes are predetermined once you have a heart attack.”
He agreed with Ms. Jacoutot, who emphasized that the program’s benefits are as much psychological as physiological. “Most people.” she said. “tend to have a lot more confidence when they get through the program. and that. I think. is just as important as the physical improvement. . . . It’s very comforting for the family as well as for the patient to see how much the patient can do safely.”
“You know what you’ve been through.” Mr. Nini added. “and you wonder sometimes whether or not you will get back to somewhat normal. physically and mentally. It’s amazing how in a short period of time these things change and your negative outlook becomes very positive.”
MEDICAL PERSONNEL involved with the program are not surprisingly, also enthusiastic about it. Dr. Rogelio Pine, who initiated the program and describes it as “reeducation and rearrangement of priorities.” said that the AHA and the American College of Cardiology approve of this type of program as treatment for cardiac patients; physicians who consider it ineffectual are usually specialists in an area other than cardiology.
Dr. Pine has found that comparisons of prc- and post-rehabilitation stress tests reveal that most patients improve their cardiovascular capacity. Future plans for the program are directed toward more scientific measuring of patient progress. Physicians hope, for example to use cardiopulmonary stress tests to measure oxygen consumption as well as heart function.
DR. STEVEN LEVINE. a cardiologist with the Princeton Medical Group who shares responsibility for structuring the program, thinks that the danger of inactivity is much greater than that of exercise in a structured and supervised environment. Many patients, he observed, are handicapped not by heart disease but by the limitations some physicians place upon patient activity.
Dr. Levine commented that at a recent ACC meeting two physicians debated the necessity for a formal rehabilitation program after a heart attack. The doctors agreed that an exercise program was necessary, but disagreed on whether the program must take place at a hospital or can be carried out at home. The controversy is economic; insurance companies question whether they should have to pay for programs to motivate patients.
ASSESSING THE EXERCISE and maintenance program. Ms. Jacoutot noted that rare cases of increased chest pain or lightheadedness have occurred, but no cardiac arrests or “codes” have taken place.
“We lay the foundation.” she said. “It’s up to the pattern to continue, and most patients do so. Dr. Pine. in fact. emphasizes that the maintenance part of the program. the permanent changing of unhealthy habits. may be the most important part of rehabilitation.
Ms. Jacoutot acknowledged that measuring the benefits in terms of life prolongation is difficult, but said, “We can say that it improves the quality of life. What I would truly lice to see is primary prevention. people starting to do these things before the heart attack